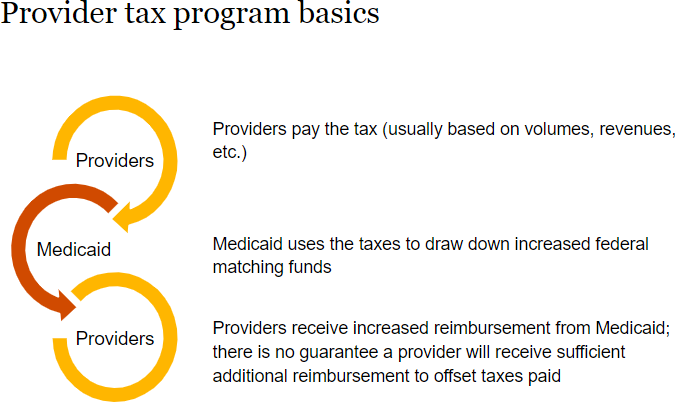
When CMS approval is delayed beyond a provider tax program’s scheduled start date, the approval granted typically is retroactive to the start date. For example, a program that was scheduled to begin on October 1 that is not approved until the following March will often mean that providers will receive a lump-sum payment in March or April that includes amounts retroactive to October 1. If the start date and the approval date fall within different financial reporting periods, questions can arise regarding the accounting for supplemental payments approved that are attributable to a prior reporting period.
This section discusses situations when the approval is received after financial statements for the prior period have been issued (or became available to be issued). If the approval is received during a reporting period’s subsequent events period, special considerations apply that are discussed in
HC 5.3.4.2When CMS approval for a program is retroactive to a date in a prior reporting period, the accounting differs depending on whether the estimate of the transaction price for services provided to Medicaid patients in the prior reporting period was constrained due to uncertainty regarding the CMS approval, as discussed in
HC 5.3.2.
If that estimate was constrained, the supplemental payments retroactively approved that are attributable to the prior period(s) would be accounted for as revenue of the period in which the constraint was removed, as required by
ASC 606-10-32-14 and
ASC 606-10-32-43 (i.e., as a change in the transaction price for the services provided in the prior period).
ASC 606-10-32-14
At the end of each reporting period, an entity shall update the estimated transaction price (including updating its assessment of whether an estimate of variable consideration is constrained) to represent faithfully the circumstances present at the end of the reporting period and the changes in circumstances during the reporting period. The entity shall account for changes in the transaction price in accordance with paragraphs 606-10-32-42 through 32-45.
Excerpt from ASC 606-10-32-43
An entity shall allocate to the performance obligations in the contract any subsequent changes in the transaction price on the same basis as at contract inception.… Amounts allocated to a satisfied performance obligation shall be recognized as revenue, or as a reduction of revenue, in the period in which the transaction price changes.
Conversely, if that estimate was not constrained, an estimate of revenue associated with the portion of the supplemental payments attributable to the prior period would have been included in revenue of the prior period (through provisional payments received and/or accruals made). Any difference between the amount estimated for the prior period and the amount actually received for the prior period in connection with the approval is reflected in the period the approval is received as a change in the transaction price associated with the prior period services. Example HC 5-2 illustrates the application of this model.
EXAMPLE HC 5-2
Accounting for retroactive CMS approval received in a subsequent reporting period
Hospital is located in a state that applied to CMS for approval of a new provider tax program that was scheduled to begin on October 1, 20x0. Hospital expects to be entitled to lump sum supplemental payments of $250,000 in each of its quarters ending December 31, 20x0, March 31, 20x1, June 30, 20x1, and September 30, 20x1, based on modeling done by the state. Historically, Hospital’s Medicaid patient base has stayed relatively consistent through the reporting year. During November 20x0, while it awaited CMS approval, the state made provisional payments to Hospital of $100,000 with the condition that if the program is not approved by CMS, the funds must be returned to the state. As of December 31, 20x0 (the close of Hospital’s fiscal year), CMS approval had not been received.
Due to the uncertainty regarding the program’s approval, Hospital constrained its estimate of revenue associated with services provided to Medicaid patients in the year ending December 31, 20x0 to exclude any amounts expected to be received from the provider tax program attributable to services rendered in that quarter. Thus, its financial statements for the fiscal year did not include any revenue from the provider tax program for services rendered to Medicaid patients during the first three months of that program. As a result, the $100,000 provisional payment received was reported as a refundable advance (a liability).
Hospital issued its financial statements for the year ended December 31, 20x0 on February 15, 20x1. Five days later (on February 20, 20x1), CMS approved the provider tax program retroactive to October 1, 20x0.
On March 1, 20x1, Hospital received a $150,000 lump sum payment from the state to catch up the supplemental payments to which Hospital was entitled for the fiscal ended December 31, 20x0.
How would Hospital account for the payment?
Analysis
The uncertainty associated with the CMS approval was resolved on February 20, 20x1 and thus, the constraint on the estimate of variable consideration attributable to the provider tax program was no longer needed. According to ASC 606-10-32-14, this is a change in transaction price associated with services provided to Medicaid patients in 20x0 that would be reported in the period in which the constraint was lifted (i.e., the quarter ended March 31, 20x1). Hospital would make the following accounting entries on February 20, 20x1:
Due from Medicaid |
$150,000 |
Refundable advances |
$100,000 |
Patient service revenue |
$250,000 |
To reflect approval of provider tax program and anticipated receipt of catch-up payment.
Hospital would then make the following entry on March 1, 20x1:
|
Due from Medicaid |
$150,000 |
To reflect catch-up payment received.
If Hospital had not constrained the estimate of variable consideration at December 31, 20x0 (for example, if the amount of revenue was deemed insignificant or if the pending approval pertained to renewal of an existing program, rather than approval of a new program), the accounting in March 20x1 would have been significantly different. In that scenario, Hospital would have included $250,000 of patient service revenue in its financial statements for the fiscal year ended December 31, 20x0. The $100,000 cash payment received in November would have reduced the corresponding receivable for services rendered and a remaining receivable from the Medicaid program of $150,000 would have been reflected on the December 31, 20x0 balance sheet. In that scenario, Hospital’s accounting entries upon receipt of the $150,000 payment on March 1, 20x1 would have been:
|
Due from Medicaid |
$150,000 |
To reflect receipt of catch-up payment.
 View image
View image